
It’s 1996. The doctor has bad news for Doug Olson. He’s just been diagnosed with chronic lymphocytic leukemia, one of the most common types of blood cancer in adults. Fast-forward to 2010 – his cancer is still not under control despite years of chemotherapy, and he’s running out of options. He decides to join a new clinical trial testing an experimental cancer treatment: genetically modifying a patient’s own immune cells so that they can kill cancer cells. Scientists called this “CAR T-cell therapy”.
Miraculously, Doug’s cancer completely disappeared [1]. This success led to further clinical trials, research, and the approval of the first CAR T-cell therapy in 2017 as well as 5 more CAR T-cell therapies targeting other blood cancers. In 2020, Doug’s blood was studied again, and scientists found that his modified immune cells were still patrolling his body, killing any cancer cells that appeared again [2]. His doctors said his cancer was essentially cured.
Remarkable, isn’t it? Right now, many of the sickest cancer patients are getting invaluable extra years of life with CAR T-cell therapy. This video will explain how this treatment works and what the future holds for this revolutionary new therapy.
Background
CAR T cells are genetically modified versions of T cells, which are immune cells with a variety of functions, one of which being the ability to target and kill infected cells. To understand how CAR T cells work, we need to first understand how T cells get activated during an infection.
T cell activation must be a tightly controlled process because unnecessary activation of T cells without infection can lead to autoimmune disease and damage to healthy tissues. To prevent this, T cells must get two signals to become fully activated. This is going to get a bit technical with lots of different receptors, so bear with me – it will help explain how the CAR T cell works.
The first signal involves the T cell receptor, a fascinating structure that T cells use to detect pathogens. Specifically, they recognize chunks of a pathogen, which are called “antigens”, like part of a protein from a virus. These receptors slightly differ in structure between T cells, which allows different T cell receptors to bind to different antigens. These antigens aren’t just floating around though – T cell receptors are picky because they only bind the antigen if they are held by a special receptor called an MHC molecule. The MHC molecule is on another cell, like a dendritic cell or another special antigen-presenting cell. The interaction between the T cell receptor recognizing its specific antigen on the MHC molecule is the first signal, which activates the T cell receptor signaling area called CD3ζ.
The second signal is called a costimulatory signal and acts like a confirmation signal, double-checking that the body is indeed under attack and the T cell should be activated. This second signal is usually activation of the signaling area of a receptor called CD28, but scientists have discovered many other co-stimulatory receptors, shown here.
When both signals are received, only then can the T cell activate and multiply. One type of T cell, called a killer T cell, will now look for infected cells to destroy. How does it know which cells are infected? It uses its T cell receptor and looks for cells that have the pathogen antigen on their MHC molecules, meaning there is pathogen inside the cell, and forces the infected cell to self-destruct, a process called apoptosis. After the infection is cleared, memory T cells will lie dormant and become reactivated if the pathogen returns. You are now immune to that pathogen.
The incredible ability of T cells to recognize a particular antigen, kill infected cells with that antigen, and create long-term immunity, made scientists wonder if we could take advantage of this feature to create T cells that can recognize cancer-specific antigens, kill cancer cells, and essentially, cure cancer. After decades of research, scientists made the idea of a modified cancer-killing T cell a reality: this is the CAR T cell.
Mechanism
CAR is an abbreviation for “Chimeric Antigen Receptor”. Much like the mythological Greek monster the Chimera, a combination of a lion, a goat, and a snake, the chimeric antigen receptor is also a combination of different receptors that allows the CAR T cell to recognize cancer proteins on the surface of cancer cells. This interaction activates the CAR T cell to destroy cancer cells in a similar method of how killer T cells destroy infected cells.
How does this work? This special receptor is made of three sections, or “domains”. The first part is the binding domain, which is designed to bind and recognize the antigen of interest. The problem with a regular T cell receptor is that it only binds antigens if they are displayed on an MHC molecule. It cannot directly recognize a surface protein on a cancer cell. To overcome this limitation, scientists decided to use special proteins from B cells called antibodies – specifically, the arms of the antibody, which can be designed to bind to almost any protein. By using one of those arms as the binding domain, the receptor can now recognize cancer surface proteins.
When this receptor binds to the cancer protein, it needs to activate the T cell, so it needs a signaling domain. Remember – a T cell needs both the T cell receptor signal and a second co-stimulatory signal to activate, so scientists have added the signaling domains from CD3ζ and CD28 to the end of the receptor. There’s currently ongoing research on which co-stimulatory molecule to use, with different combinations of co-stimulatory signals providing varying effectiveness in different cancer types.
Lastly, to connect the two domains inside and outside the cell membrane, a transmembrane domain from another protein is used. The segment connecting the binding and transmembrane domains is called a hinge or spacer, which allows the binding domain to be flexible when binding to the antigen, increasing its chances of successful binding. And with these three domains, we’ve got ourselves a chimeric antigen receptor that binds to cancer proteins and activates the CAR T cell.
So how do we modify T cells to have these special receptors? Since this entire receptor is a protein, we can take the different DNA sequences encoding the different parts, join them up, and deliver into T cells, usually by a disarmed virus. First, a special machine filters out white blood cells from patient blood, a process called leukapheresis. Then, in the laboratory, the T cells are isolated from the white blood cells, and genetically modified. The modified T cells that express the receptor are selected and stimulated to proliferate into millions of cells, then transfused back into the patient to start eliminating cancer cells. This entire process takes around one month.
As of 2023, there are six approved CAR T cell therapies for blood cancers [4]. Four of them target the protein CD19 to treat B cell leukemias and lymphomas, and the other two target BCMA to treat multiple myeloma. CD19 and BCMA are proteins also found on healthy B cells, so B cells are also destroyed during CAR T cell therapy and patients need careful monitoring and replenishing of antibodies after treatment.
CAR T cell therapies are currently used only after other treatments have failed, and they still show remarkable success in these blood cancers. For example, in a recent Phase III randomized clinical trial of 386 patients with relapsed or treatment resistant multiple myeloma, patients who received the CAR T cell therapy idecabtagene vicleucel had higher rates of patients responding to treatment, higher rates of complete cancer elimination, and a longer time being cancer free compared to current standard therapies [5]. These impressive findings are encouraging scientists to test CAR T cell therapy as an initial treatment rather than a last resort, with promising results [6].
We are also starting to realize that patients can be cancer free for years after CAR T cell therapy, like in Doug Olson’s case. Scientists think that this happens when some CAR T cells turn into other T cell types or behave like memory T cells. They then patrol the body for cancer cells for many years after transfusion [2]. This really is an incredible “living” drug!
Side Effects
However, this treatment isn’t without side effects. Aside from depleting B cells, activated CAR T cells can also activate other immune cells, resulting in the release of immune signaling molecules called cytokines. The widespread activation of CAR T cells and other immune cells results in cytokine release syndrome, which can range from a mild fever, which happens in most patients, all the way to organ failure, which is rare but life threatening. The severity of this side effect is dependent on the amount of cancer originally in the body – more cancer cells will activate more CAR T cells, resulting in more cytokines released and a greater severity of cytokine release syndrome. Another rare side effect occurs when the cytokines also damage the blood-brain barrier and the brain itself, resulting in severe neurological symptoms. This is called immune effector cell-associated neurotoxicity syndrome. These two severe side effects require careful monitoring and treatment with immune suppressants, but most patients are able to recover from this [7].
The Future of CAR T Cell Therapy
What does the future hold for CAR T cell therapy? The most fascinating aspect of this therapy is really the potential of genetic bioengineering. Here are some cool ideas being tested in the lab and in clinical trials [8].
To make an even more specific CAR T cell receptor, the receptor could be modified to recognize two different proteins, and both need to be activated for killing, called a “Tandem” car.
Research is also ongoing to design CAR T cells that work in solid tumors. Solid tumours are resistant to CAR T cell therapy because they can express molecules that activate off-switches on T cells. “Armored” CAR T cells are genetically modified to remove these off-switches, protecting CAR T cells from being disarmed, so they have a better chance of destroying solid tumors.
Conversely, “self-destruct” CAR T cells are genetically modified so they express an apoptosis protein that is only activated in response to a drug. The idea is, if side effects are out of control, a doctor can inject the self-destruct drug and the CAR T cells will die, stopping the side effects.
Lastly, CAR T cells have to be made from a patient’s own T cells to prevent transplant rejection. Right now, scientists are working on creating a “universal” CAR T cell that can be transfused into anyone and essentially used right off the shelf like other medications, which could dramatically reduce manufacturing time and the cost of this highly expensive therapy.
These are just a sample of “power-ups” for CAR T cells, with many more being developed and researched, as well as other creative ideas such as using other types of immune cells [9] or using CAR T cells to prevent autoimmune disease [10] – more on this in the description below.
While there are still challenges to overcome, including better management of side effects, lowering costs [11], and targeting more types of cancer like solid tumors, CAR T cell therapy represents a breakthrough in cancer therapy, offering hope to patients who previously had no treatment options left. Continued research will improve this relatively new therapy into an even more effective tool in the fight against cancer.
Thanks for watching. If you have requests for future video topics, I’d love to hear them! And as always, see you next time on Medicurio.
References
- Kalos, M., Levine, B. L., Porter, D. L., Katz, S. I., Grupp, S. A., Bagg, A., … & June, C. H. (2011). T cells with chimeric antigen receptors have potent antitumor effects and can establish memory in patients with advanced leukemia. Science Translational Medicine, 3(95). https://doi.org/10.1126/scitranslmed.3002842
- Melenhorst, J. J., Chen, G. M., Wang, M., Porter, D. L., Chen, C., Collins, M. A., … & June, C. H. (2022). Decade-long leukaemia remissions with persistence of CD4+ CAR T cells. Nature, 602(7897), 503-509. https://doi.org/10.1038/s41586-021-04390-6
- Jayaraman, J., Mellody, M., Hou, A. J., Desai, R. P., Fung, A. W., Pham, A. T., … & Zhao, W. (2020). Car-T design: elements and their synergistic function. EBioMedicine, 58, 102931. https://doi.org/10.1016/j.ebiom.2020.102931
- Mazinani, M. and Rahbarizadeh, F. (2022). Car-T cell potency: from structural elements to vector backbone components. Biomarker Research, 10(1). https://doi.org/10.1186/s40364-022-00417-w
- Rodriguez-Otero, P., Ailawadhi, S., Arnulf, B., Patel, K., Cavo, M., Nooka, A. K., … & Giralt, S. (2023). Ide-cel or standard regimens in relapsed and refractory multiple myeloma. New England Journal of Medicine, 388(11), 1002-1014. https://doi.org/10.1056/nejmoa2213614
- Locke, F. L., Jacobson, C. A., Perales, M., Perales, M., Oluwole, O. O., Ghobadi, A., … & Westin, J. R. (2022). Axicabtagene ciloleucel as second-line therapy for large B-cell lymphoma. New England Journal of Medicine, 386(7), 640-654. https://doi.org/10.1056/nejmoa2116133
- Morris, E. C., Neelapu, S. S., Giavridis, T., & Sadelain, M. (2021). Cytokine release syndrome and associated neurotoxicity in cancer immunotherapy. Nature Reviews Immunology, 22(2), 85-96. https://doi.org/10.1038/s41577-021-00547-6
- Fesnak, A. D., June, C. H., & Levine, B. L. (2016). Engineered T cells: the promise and challenges of cancer immunotherapy. Nature Reviews Cancer, 16(9), 566-581. https://doi.org/10.1038/nrc.2016.97
- Pan, K., Farrukh, H., Chittepu, V. C. S. R., Xu, H., Pan, C., & Zhu, Z. H. (2022). Car race to cancer immunotherapy: from car t, car nk to car macrophage therapy. Journal of Experimental & Clinical Cancer Research, 41(1). https://doi.org/10.1186/s13046-022-02327-z
- Arjomandnejad, M., Kopec, A. L., & Keeler, A. M. (2022). CAR-T regulatory (CAR-Treg) cells: engineering and applications. Biomedicines, 10(2), 287. https://doi.org/10.3390/biomedicines10020287
- Lin, J., Muffly, L., Spinner, M. A., Barnes, J., Owens, D. K., & Goldhaber-Fiebert, J. D. (2019). Cost effectiveness of chimeric antigen receptor T-cell therapy in multiply relapsed or refractory adult large b-cell lymphoma. Journal of Clinical Oncology, 37(24), 2105-2119. https://doi.org/10.1200/jco.18.02079
Extra Information
Doug Olson’s Story
You can read more about his story published in the New York Times as well as the initial paper describing the clinical trial he was in back in 2010, and the follow-up study done 10 years later.
The Complex Interaction between the TCR, antigen, and the MHC molecule
The interaction between the MHC molecule and the T cell receptor (TCR) is slightly more complex than what was shown in the video. There are two classes of MHC molecules, Class I and II. Class I MHC molecules are found on all cells with a nucleus and present antigens that are found inside cells, which can either be from normal cell proteins or intracellular pathogens like viruses. Class II MHC molecules are only found on special cells called antigen presenting cells, like dendritic cells, macrophages, and B cells, and generally present antigens that are from normal cell proteins found outside cells or from extracellular pathogens like bacteria. There are also two types of T cells that recognize these two different classes. CD8 killer T cells recognize MHC Class I using their TCR, while CD4 helper T cells recognize MHC Class II. CD8 and CD4 are co-receptor surface proteins on T cells that work alongside the TCR to bind to MHC Class I and II, respectively. This distinction is important for making sure the right immune cells are activated and that infected cells are killed. You can read more about this interaction in this review.
What’s the Fuss About Co-Stimulation?
T cell activation needs to be very tightly controlled, so there are multiple checks during the process. One of these is the activation of co-stimulatory receptors, which should only occur when there is an ongoing infection. This is important because if a TCR recognizes a regular cell protein antigen by accident, it might now start attacking normal cells. However, without a co-stimulatory signal to go alongside it, the T cell will either die through apoptosis or go into hibernation, or “anergy”, preventing autoimmune disease. CD28 is the classic receptor on T cells, which recognizes the B7 protein found on antigen presenting cells, and the B7 protein only is expressed during infection. 4-1BB and OX40 are some of the many other co-stimulatory molecules being studied. The first generation CAR T cells only had CD3ζ, and these CAR T cells did not get activated very well and died shortly after. Once scientists began adding a co-stimulatory domain to the chimeric antigen receptor (second generation CARs), they were amazed at how effective CAR T cell therapy was. Of the approved CAR T cell therapies in 2023, CD28 or 4-1BB are used as co-stimulatory signals. CD28-containing CAR T cells have a more rapid effect but also wear out quickly, while 4-1BB containing CAR T cells have a weaker effect but longer duration and lower risk of side effects (reference). Some of the newest generation CAR T cells are including not just one, but multiple co-stimulatory signaling domains (3rd generation CARs) to see if these can create even better CAR T cells.
There are also “negative-regulator” receptors like CTLA-4 and PD1, which when activated will result in deactivation of the T cell. New cancer therapies target these negative-regulator receptors to prevent T cells turning off, so they are better at killing cancer cells. “Armored” CAR T cells will genetically remove these receptors, while checkpoint inhibitors, another type of cancer immunotherapy, will prevent these negative-regulator receptors from being activated.
The Natural Cancer-Killing Ability of the Immune System
When cells accumulate multiple mutations in genes that control cell replication, they can begin to undergo uncontrolled cellular proliferation, resulting in cancer. These mutations can occur whenever a cell replicates, when there is DNA damage, or can be inherited from your parents. A scary thought is that we probably all have pre-cancerous cells inside us right now, but our immune system is regularly patrolling the body to eliminate these before they get out of control. T cells can recognize antigens from mutated proteins and destroy them, while another immune cell called Natural Killer (NK) cells can also eliminate cells that are stressed from the mutations and are expressing stress proteins. However, these defenses are not 100% effective, and certain mutations can allow the cancer cell to escape detection, resulting in cancer and the need for treatment.
New Ideas for CAR T Cells
“Tandem” CARs, “Armoured” CARs, and “Self-Destruct CARs” are just some of the many ideas scientists have come up with (as well as other vehicle puns). Currently, there is ongoing research to make CAR T cells that are better at killing, home to tumours, and avoid healthy cells. Scientists are also modifying other immune cells to express CARs and using CAR T cells in other diseases, like autoimmune diseases, which is really exciting.
“T cells Redirected for antigen-Unrestricted Cytokine-initiated Killing”, or “TRUCKs”, are 4th generation CAR T cells that are designed to recognize cancer proteins and then release multiple cytokines when activated, which facilitate tumour killing. “Self-driving” CARs have another receptor that binds to molecules released by tumours, which allows them to home into tumours and start killing cancer cells. “Safety” CARs have an additional CAR that recognizes proteins found on normal cells, and if this receptor is activated, it shuts down the T cell, preventing the CAR T cell from killing normal cells by accident.
Universal CAR T cells are a very hot topic because we need to make this therapy more accessible for everyone. When we transfuse or transplant anything, we need to make sure that things like “blood types” match between the donor and the recipient, otherwise the immune system will attack the new cells or organ because it doesn’t recognize the transplant as part of the body. MHC molecules are another surface molecule that needs to match between donor and recipient (there are many variants of MHC molecules), so scientists are trying to see if they can genetically remove some of these person-unique markers from CAR T cells so that they don’t trigger the immune response in the person receiving CAR T cell therapy. This is a lot easier said than done, which is why CAR T cells are still made from a patient’s own cells despite its exorbitant costs.
There is also ongoing research with genetically modifying NK cells and macrophages, which also can destroy cells, to express chimeric antigen receptors so they can recognize and destroy cancer cells. Surprisingly, CAR T cells are also being investigated in treating autoimmune disease. Regulatory T cells (Tregs) are a type of T cell that, instead of killing cells, releases cytokines that turn off other nearby immune cells. Scientists are designing CAR Tregs to recognize antigens in an organ that is under attack, like the pancreas in Type 1 diabetes. When these CAR Tregs reach the pancreas, they will get activated and shut down the surrounding immune cells, stopping the autoimmune reaction and saving the pancreas.
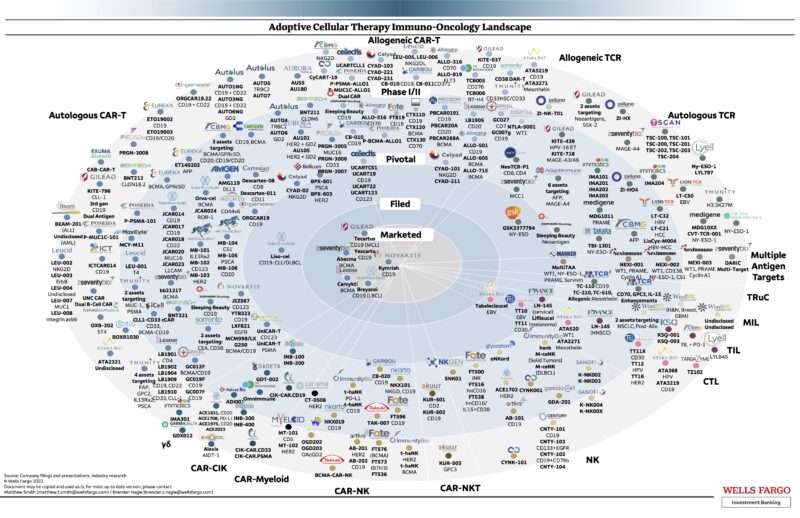
This field is really in its early stages, so there are lots of opportunities for creative people with an understanding of immunology to really make a difference in not only cancer but other diseases as well! This chart from 2022 is a snapshot of all the CAR therapies under development (by Matthew Smith from Wells Fargo):
Hypogammaglobulinemia, CRS, and ICANS
Hypogammaglobulinemia, which essentially means “low antibody levels”, is a common feature of the current approved CAR T cell therapies. This is because CD19 and BCMA are expressed on healthy B cells as well, so they are also killed by CAR T cells. B cells produce antibodies, so patients will often have low levels of antibodies after CAR T cell therapy (in fact, detecting low antibody levels and low B cell levels in the blood are indications that the CAR T cell therapy is working). Patients can live without B cells, but they will need frequent injections of intravenous immunoglobulins (IVIG), which is essentially purified antibodies from another person, to replenish their own antibody levels. Otherwise, without antibodies, patients are more likely to get potentially lethal infections.
Cytokine Release Syndrome (CRS) is a phenomenon of increased levels of inflammatory cytokines in the blood, resulting in low blood pressure and organ dysfunction. A more severe version of this disease is called hemophagocytic lymphohistiocytosis (HLH), where essentially the body’s immune cells start eating its own red blood cells, release massive amounts of cytokines (a “cytokine storm”), and destroy its own organs. The main cytokine that initiates all of this is Interleukin-6, which is usually released from activated macrophages. The good news is, we have treatments that block IL-6 from working, such as tocilizumab (you might have heard of this drug for severe COVID-19, which is a similar inflammatory disease in part mediated by IL-6).
Immune effector Cell-Associated Neurotoxicity Syndrome (ICANS) is another side effect mediated by cytokines like IL-6 that leak into the brain, and again is treated by tocilizumab and steroids to dampen the immune response. Scientists still aren’t sure why the brain is damaged, but interestingly, some cells that make up the blood brain barrier also have CD19, so one hypothesis is that CAR T cells also attack these barrier cells, resulting in a leaky barrier that allows cytokines to pass through (reference). Patients with ICANS will have altered consciousness, difficulty speaking and understanding, and issues with moving, and can progress to seizures, coma, and possible death if untreated by immune suppressants.
Thank You, Alpacas, For Your Nanobodies
You read that right. The camelids (camels, llamas, vicunas, guanacos, and alpacas) have a fascinating immune system because they do not have antibodies like us, but smaller versions called nanobodies (turns out that sharks have them too!). Instead of two arms, nanobodies only have one arm. Because they’re smaller, they have better solubility, more flexible, can sneak in and bind to hard-to-reach antigens, and are more easily synthesized and purified. Nanobodies are currently used in molecular imaging, drug delivery, and recently, Carvykti is the first approved CAR T cell therapy to use nanobodies instead of antibodies. So alpacas are not just fluffy, but they also are advancing science and saving people’s lives!
Excellent video and article! It really helps me a lot since I am planning to switch to this industry. The content is very clear, using simple words to demonstrate complex concepts and mechanisms. Thanks a lot !